
There is a lot of momentum around primary care medical home (PCMH) and team based care. In the various pilots and implementation, we see around the country, there is no one “right” answer for team size and configuration, panel size per team member, etc.
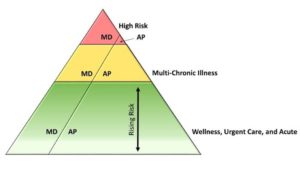
Most teams include some contribution of behavioral health, social work, case management, pharmacy, nutrition, nursing, nurse educators, medical assistants, and health coach. One of the more compelling models we have seen is the Dyad/Teamlet model, where the extended team supports not just a physician, but a physician/AP dyad. The dyad shares a panel of patients (larger panel than a single provider). The highest risk/post hospitalization patients in the panel are seen mostly by the physician, while the AP mostly sees wellness and urgent care visits. Chronic disease management is a shared responsibility. As the patient risk moves up the pyramid, the visits are more commonly seen by the physician. This model can be seen in the image attached.
This model has several benefits:
- The combined capacity of two providers means it is more likely the patient will see a provider who is familiar with their situation
- The two providers can share a cohort of exam rooms—each using the first available for a visit—leading to more efficient use of rooms
- More efficient use of the extended care team (social work, pharmacy, etc.), since they are supporting a larger panel
- Greater bonding of the patient with the extended care team
What is your experience? Is two better than one?
By Wendy Weitzner | February 2016